You finally decided to try HRT. Now the patches are running out.
Editorial note
LAKEHAUS Health articles are written for education and clarity. We aim to separate useful evidence from wellness theater, and we update articles when better information becomes available. This content is not medical advice and is not a substitute for care from a qualified clinician.
The Estrogen Reckoning
Why the patch shortage is exposing the gaps between medical consensus and pharmaceutical infrastructure
For more than two decades, estrogen therapy existed in a peculiar medical purgatory—a treatment simultaneously vilified and essential, unavailable to many who needed it most. The 2002 Women's Health Initiative study, with its alarming associations between hormone replacement and breast cancer risk, triggered an exodus. The FDA affixed a black-box warning, that most serious of pharmaceutical designations, and usage plummeted below 5%. A generation of physicians, trained in an era of caution, simply stopped prescribing. And a generation of women, navigating the volatile terrain of perimenopause without pharmaceutical support, suffered quietly.
But medicine, when practiced properly, is self-correcting. Rigorous re-examination of that landmark study revealed critical flaws: the research focused on specific synthetic formulations, administered to older populations, in protocols that couldn't responsibly be generalized to all women at all life stages. The data, in short, had been misapplied to the wrong patients.
The Pendulum Swings
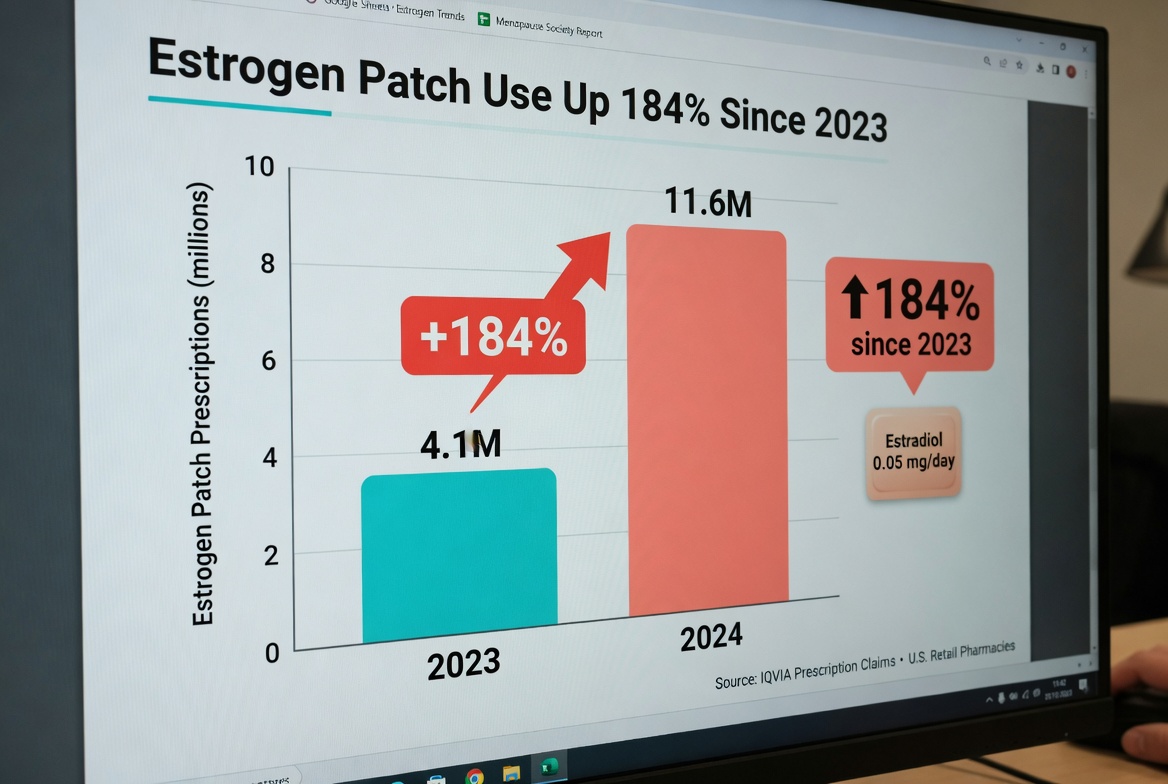
The rehabilitation was swift and, by many measures, overdue. Last July, FDA Commissioner Marty Makary began publicly characterizing hormone therapy as potentially "lifesaving"—a remarkable semantic shift from "dangerous" to "protective." By November, the black-box warning was removed. And demand, predictably, exploded. Estrogen patch prescriptions have surged 184% since 2023, with a 26% spike in the two months following the November announcement alone.
Herein lies the paradox: estrogen patches are generic medications, carrying the slim profit margins that disincentivize pharmaceutical manufacturers from rapidly scaling production infrastructure. The result is a shortage that industry insiders suggest could persist for up to three years. Women who have finally found relief are hunting across multiple pharmacies, switching formulations mid-protocol, or worse, discontinuing abruptly—only to have symptoms return with devastating intensity. The cruelty of finally receiving validation for a treatment you need, then discovering the supply chain cannot accommodate your prescription, is not lost on anyone navigating this landscape.
Navigating the Gap
If you are currently staring at an empty pharmacy shelf, know this: the scarcity is systemic, not personal. Call ahead before making the trip. More importantly, understand that transdermal patches, while elegant in their simplicity, represent only one delivery mechanism among several viable options.
Alternatives to Consider
- Gels and sprays offer comparable absorption without the adhesive variables
- Vaginal rings provide localized delivery with systemic benefits
- Telehealth platforms with compounding capabilities are filling supply gaps
- Compounded formulations require specific physician consultation regarding standardization
Telehealth services connected to compounding pharmacies have emerged as crucial stopgaps, though with important caveats: these customized formulations lack FDA review as finished products, necessitating a detailed conversation with your clinician about quality assurance and batch consistency.
And if a practitioner insists that patches represent the only "correct" method of delivery, it may be worth seeking a second opinion. Menopause medicine, perhaps more than any other specialty, demands individualized protocols. Biochemistry varies; absorption rates differ; lifestyle factors influence compliance. The best therapy is the one you can consistently access and tolerate.
The Hype Cycle
Yet we must address the distorting lens of cultural enthusiasm. The rehabilitation of HRT is largely scientifically warranted; the hype machine surrounding it is not. Social media platforms, populated by celebrities and wellness influencers without medical credentials, have generated a pressure toward universal adoption that mirrors the previous pressure toward universal avoidance. Neither extreme serves women well.
Not every woman requires hormone therapy. Not every candidate is suited for it. The rush toward one-size-fits-all prescribing—driven partly by influencers and partly by general practitioners lacking specialized menopause training—has legitimate clinicians concerned. We have moved from "hormones are dangerous" to "hormones are essential" without adequate pause for the nuanced middle: hormones are powerful tools that require individualized risk assessment, genetic screening, and ongoing monitoring.
The Reality: The removal of the black-box warning represents scientific progress, not a fashion trend. The shortage reveals the fragility of generic drug supply chains when demand shifts rapidly. For women caught in this moment, the imperative is pragmatic flexibility—exploring alternative delivery systems, advocating for compounding options when appropriate, and resisting the binary thinking that created this crisis in the first place. The goal remains steady physiological support, not adherence to a specific delivery method. Precision medicine, after all, requires options.
